



"The Abortion Talk" for Anesthesiologists
It's time to inspire academic anesthesiologists to research abortion

Last Friday, after shoveling down a salad, I hustled onto the International Anesthesiology Research Society’s (IARS) big stage in a Denver ballroom to talk about an issue anesthesiologists are notoriously quiet on: abortion.
My co-panelist and co-authors, Drs. Ruthi Landau from New York and Caitlin Sutton from Texas, and I prepared extensively. We had the data. We could tie together the implication for the audience.
Attendees kept asking us what we would present. “Oh, we’re giving the abortion talk.” Their eyes got a little wider, and they nodded knowingly. “Good for you. We need to talk about it.”
We knew giving this talk would take bravery.

How hostile would the audience be?
Anesthesiology tends to be politically conservative, and I felt we needed to be prepared for a potentially hostile audience. Would someone get angry and make a scene at the meeting? How much misogyny would show up in the Q&A?
A group of anesthesiologists (including me) spent last summer and fall advocating for open dialog about the impact of the Dobbs decisions on anesthesiology and patient safety, which drew unprofessional comments on our society’s internal message boards.
At the recent Society for Pediatric Anesthesiology meeting, an anesthesiologist insisted on mansplaining gun violence to the pediatric intensivist who had just given a talk reviewing the terrifying data on the leading cause of death in children: gunshots.
Was that going to happen when we laid out how abortion restrictions kill and harm our patients?
Dr. Landau, a Swiss-trained East Coast anesthesiologist and researcher, introduced our topic and set the tone beautifully:
“In today’s medical, legal, and economic landscape, some conversations require courage, integrity, and cultural competence. Talking about maternal health and reproductive justice in the post-Roe world is a conversation we are compelled to have today with this esteemed community of international anesthesiologists and researchers.
We felt this is a necessary conversation to have with you.
Though perspectives may vary in the audience, and we certainly don’t have all the answers in this evolving landscape, it is with great respect and trust that we hope this will result in a just inquiry, here and beyond, and in advocacy that will help advance reproductive health and reduce racial and ethnic disparities in maternal and neonatal outcomes.” - Dr. Landau
What does the data tell us?
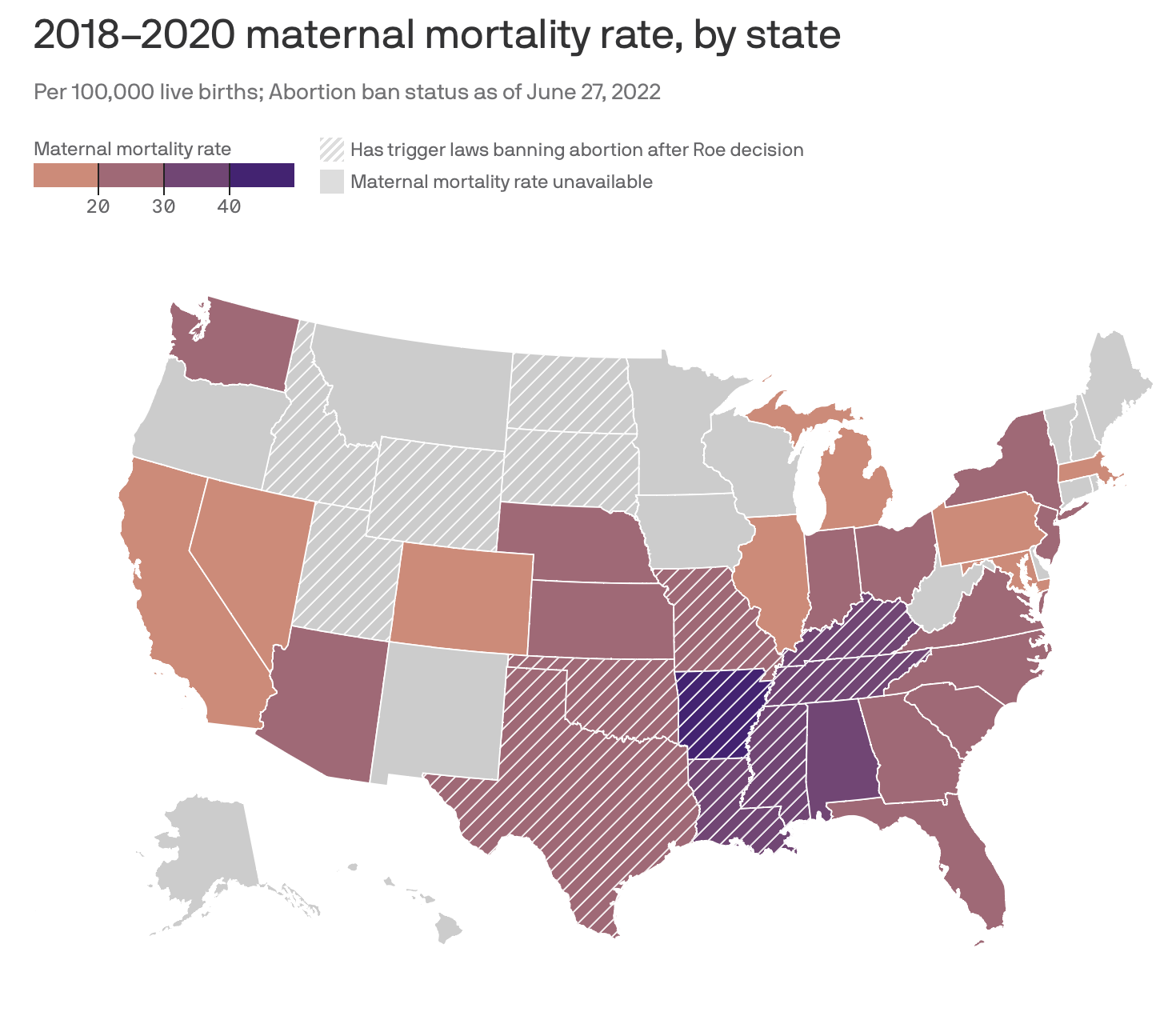
In her presentation, Ruthi laid the evidence bare. She covered international and US maternal mortality data, highlighting the US’s abysmal outcomes. The overall outcomes are terrible, but especially so for Black women. Covering this topic during Black Maternal Heath Week was particularly powerful.
She reviewed the rising popularity and safety of medication abortions, and how assaults on access to medication abortion mean more patients will seek surgical abortions - and needs access to anesthesiologists. Dr. Landau showed the audience how even before the fall of Roe, maternal mortality rates already tended to be higher in states with restrictive abortion bans. We know the data will worsen.
Ruthi did some serious heavy lifting to cover the relevant data and present it cohesively. Plus, news on the mifepristone case and new abortion regulations came out in the hours leading up to and even during our talk.
What every anesthesiologist can do today
Dr. Sutton, a Texas-based maternal-fetal anesthesiologist and bioethicist, highlighted the ways anesthesiologists can prevent pregnancies. We are pharmacology experts and know some of our medications (mainly sugammadex and aprepitant) cause hormonal birth control not to work for 1-4 weeks. What many anesthesiologists don’t know, is that patients don’t know that a “barrier contraceptive” is a condom.
Their partners will refuse to use a condom, and even suggesting a condom may get them beaten.
13–61% of women worldwide report being physically assaulted by an intimate male partner during their lives. Intimate partner violence impacts at least 25% of American women, and this abuse goes hand-in-hand with reproductive coercion.
Dr. Sutton also pointed out the role of anesthesiologists in ensuring labor and delivery patients who want tubal ligations (highly effective, permanent contraception), can get them, no matter the time of day. We need to treat these quick surgeries as urgent/emergent because 50% of patients who can’t get them at the time of delivery will be pregnant again within one year. For millions of pregnant-capable people who can not access abortion care, these are critical procedures.
Dr. Sutton covered education and a generation of anesthesiologists whose education will have major gaps. She packaged it all up in a checklist for anesthesiologists, including educational topics to be covered with trainees.
Research as Advocacy
We need doctors - including anesthesiologists - to develop a broader understanding of what advocacy can look like. I tend towards loud, public advocacy. I like to talk to journalists and write op-eds.
In a world designed for extroverts, some folks think this is the only way to make a difference. But quiet, diligent advocacy through research is immensely important and is the fuel necessary for other forms of advocacy.
My goal for the panel was to help anesthesiologists expand their horizons about what counts. Many anesthesiologists are in despair about the current state of medical care in our country.
I asked the audience to consider one question while I spoke: What research and writing might you do at the intersection of anesthesiology and reproductive healthcare?
Do not despair. Do research. Write papers.
Research on safe anesthesiology abortion? That’s advocacy.
Studying geographic access to surgical abortion and anesthesiology care? That’s advocacy.
Writing about the implications of the loss of abortion access on surgical caseloads? That’s advocacy.
Sharing how hospital policies are changing in response to state-level restrictions? That’s advocacy.
Knowledge is power.
As academics, we are in the business of generating and sharing knowledge. If you care about patients and you do research, I invite you to re-think your role in the knowledge ecosystem.
If you want to see our suggested research agenda (and all our references), they are here for you.
Thankfully, the IARS Audience Delivered
We prepared - intellectually and emotionally - to cover a crucial conversation with a potentially hostile audience. But the audience in Denver was gracious and kind. They had tough questions, but not belligerent ones. We were fortunate to have a long line of people waiting to talk to us about research opportunities and how they may determine who is safe to talk to in their own organizations. We had CA-1s through senior physicians chatting afterward.
There is so much more work to do in anesthesiology to improve reproductive healthcare. I’m glad my colleagues are awakening to this critical patient safety issue. I’m thrilled to partner with such incredible physicians and work together to spread the word of reproductive justice.